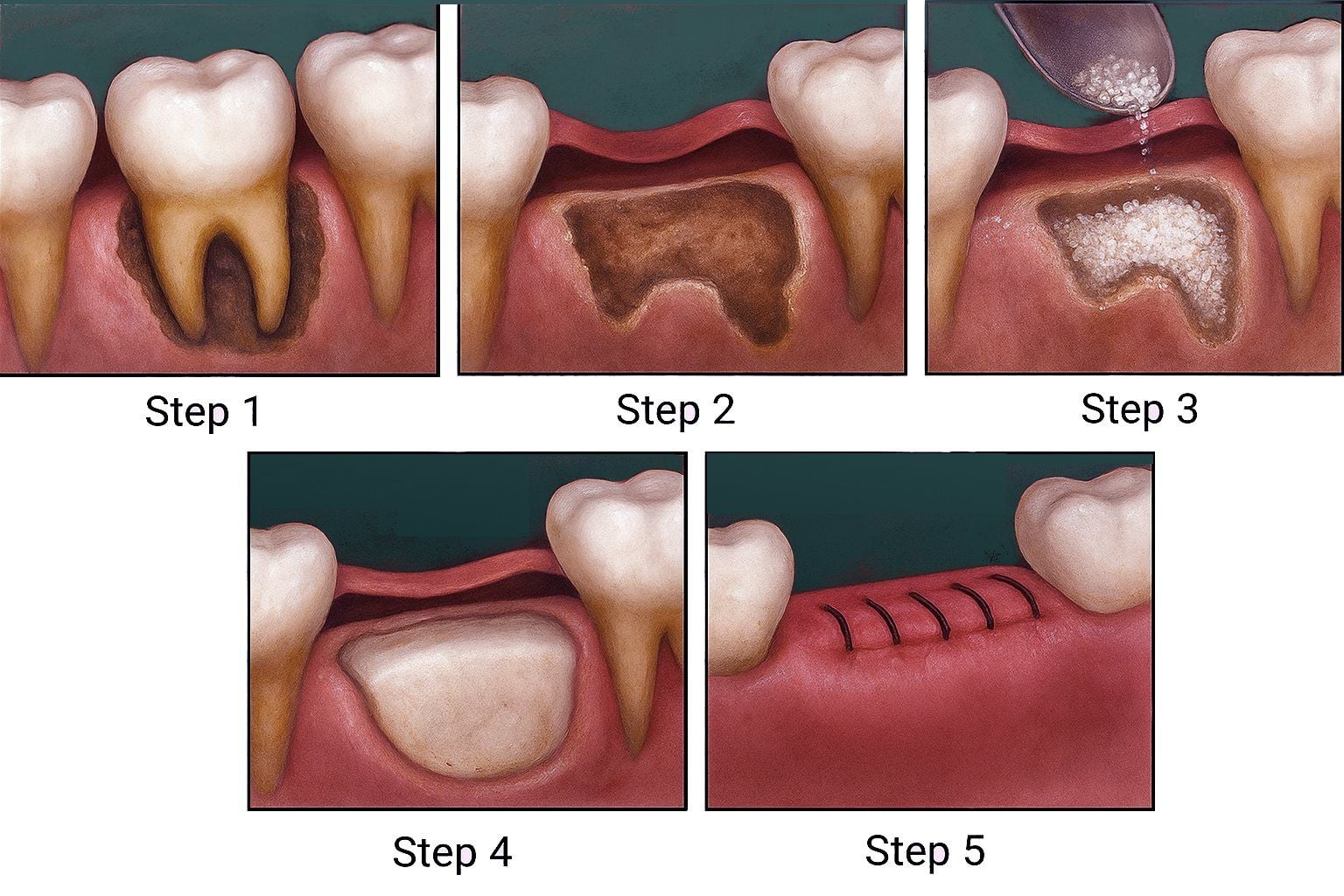
Our specialist physicians generally perform the bone graft procedure under local anesthesia with the following steps:
Examination and Planning: Radiographic examination is necessary to understand the need for a bone graft. X-rays are examined by our doctors. The patient's intraoral examination is performed, and their general/systemic medical condition is evaluated in detail. If there is no condition in the general health status that prevents oral surgery, the bone grafting procedure is planned.
Surgical Preparation: A sterile preparation is made for this procedure, which is performed in a sterile environment. To counter the risk of infection, the area where the procedure will be applied is cleaned with an antiseptic solution.
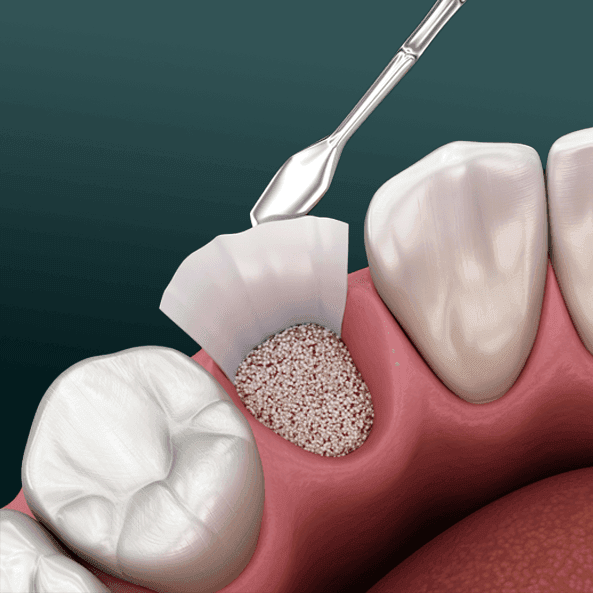
Placement of the Graft: The area where the graft will be applied is reached through a surgical procedure, and the defective area is rehabilitated with the bone graft.
Application of a Membrane: The bone graft is isolated with a barrier (membrane), and the surgical site is closed with sutures.
Healing: New bone formation is generally completed between 4 and 6 months.